
Achilles Tendonitis vs. Plantar Fasciitis — How to Tell the Difference (and Why It Matters)
Your Complete Guide to Heel Pain Diagnosis
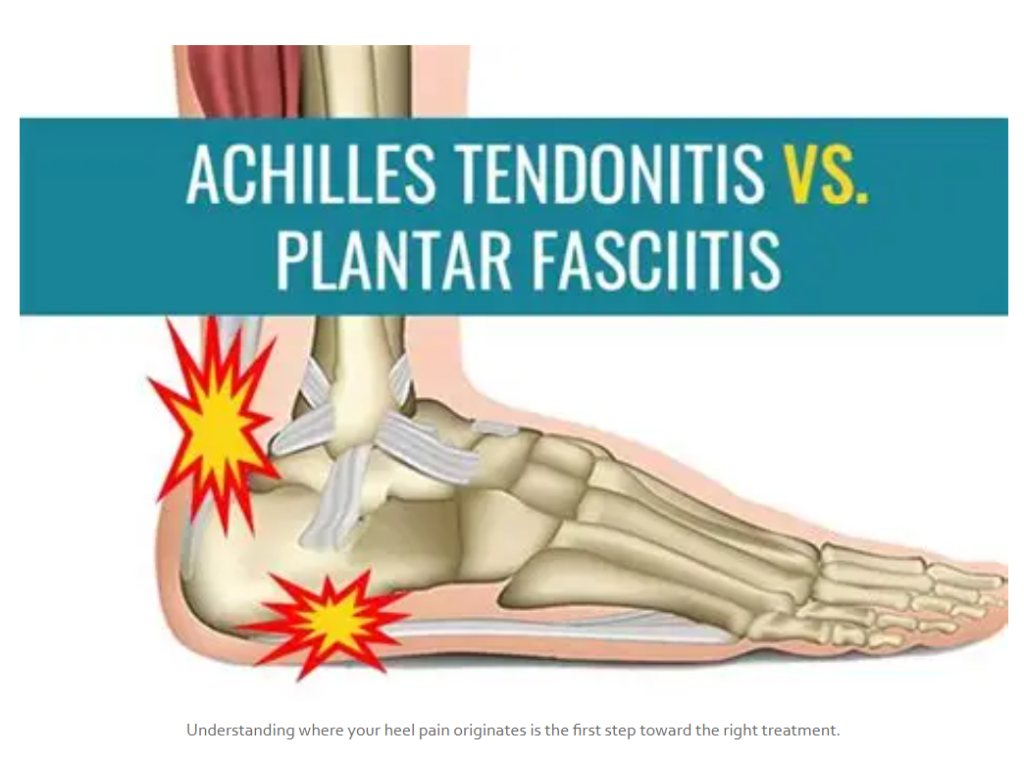
Understanding where your heel pain originates is the first step toward the right treatment.
“My heel hurts — is it achilles tendonitis or plantar fasciitis?” If you’ve typed that question into a search bar at midnight while icing your foot after a run, you’re not alone. Achilles tendonitis vs. plantar fasciitis is one of the most common diagnostic questions we hear in our Mesa, AZ clinic, and for good reason. These two conditions are the most frequent causes of heel and foot pain in active athletic adults. (aka weekend warriors aka Mesa City Pickleball Champion 2 times in a row! lol)
They share overlapping symptoms — especially that morning stiffness and heel pain — but they are fundamentally different injuries affecting different anatomical structures.
Misdiagnosis is shockingly common. As a sports performance specialist in the East Valley, we regularly see patients who have been treated for the wrong condition for months, sometimes longer.
Getting the diagnosis right is the first and most important step toward getting out of pain. This guide will give you the tools to tell the difference between Achilles tendonitis and plantar fasciitis — and explain why it matters for your recovery.
The Quick Answer — Location Tells You Almost Everything
Before we dive deep into anatomy and testing, here is the simplest way to start figuring out whether you’re dealing with plantar fasciitis or Achilles tendonitis…this is not how you really diagnose it, but an at home test to get self-care started.
- Pain at the BACK of the heel or along the tendon above the heel = Achilles tendonitis territory
- Pain at the BOTTOM of the heel or radiating into the arch = Plantar fasciitis territory
These are two completely different anatomical structures. The pain in the back of the heel vs. the bottom of the heel distinction is not subtle — it points to two separate injuries requiring two separate treatment strategies. If a provider is treating pain on the bottom of your foot as Achilles tendonitis, or pain at the back of your heel as plantar fasciitis, it is time to find a new provider.
Quick Reference |
What Is Achilles Tendonitis?
The Achilles tendon is the thickest, strongest tendon in the human body. It connects the gastrocnemius and soleus (your two primary calf muscles) to the calcaneus (heel bone), and it is responsible for every push-off motion you make — walking, running, jumping, climbing stairs.
Achilles tendonitis — more accurately called Achilles tendinopathy — is not a simple “inflammation” despite what the name implies. It is a degenerative condition involving collagen breakdown, fiber disorganization, and neovascularization (abnormal blood vessel growth) within the tendon. This happens when the tendon is subjected to repetitive overload without adequate time to repair.
There are two distinct types, and the distinction matters for treatment:
- Mid-portion Achilles tendinopathy: Occurs 1-3 inches above the heel bone, in what’s called the “watershed zone” — an area with reduced blood supply that makes it vulnerable to degeneration and slow to heal. (But only when the muscles lose their shock absorbing ability, which I’ll cover later.)
- Insertional Achilles tendinopathy: Occurs right where the tendon attaches to the heel bone. Often associated with calcifications or a bony prominence called Haglund’s deformity. (Guess what? these calcifcations and “heel spurs” aren’t a bad sign. They actually mean you are healing! Indicating less of a need for surgery.)
Achilles Tendonitis Symptoms
- Pain and stiffness at the back of the heel or lower calf
- Morning stiffness that gradually “warms up” with movement
- Pain that worsens during or after activity — running, jumping, pushing off
- Possible visible swelling or thickening along the tendon
- Difficulty with push-off during walking or running
- A tender bump or nodule you can feel along the tendon
Risk Factors (note: these are not what needs to be treated to heal)
- Sudden increases in training volume or intensity (the classic “too much, too soon”)
- Chronically tight calves and reduced ankle dorsiflexion
- Age (tendon quality decreases over time)
- Obesity or being overweight
- Fluoroquinolone antibiotics (Cipro, Levaquin) — a well-documented but underappreciated risk factor – I’ve seen this risk factor persist for up to 10 years…
What Is Plantar Fasciitis?

Plantar fasciitis (sometimes) involves micro-tearing and degeneration of the plantar fascia at its attachment to the heel bone. (But this isn’t the root cause of pain. In fact, you can keep all the changes in tissue and have zero pain. This is where everyone gets it wrong!)
The plantar fascia is a thick, fibrous band of connective tissue that runs along the bottom of the foot from the calcaneus (heel bone) to the base of the toes. It supports the arch, absorbs shock with every step, and plays a critical role in the biomechanics of walking and running.
Plantar fasciitis used to be defined as micro-tearing and degeneration of the plantar fascia at its origin on the medial calcaneal tubercle — the inside-bottom of your heel bone. But, research has recently found that there doesn’t need to be any tissue damage or inflammation to have the condition.
It is the #1 cause of pain on the bottom of the heel, affecting up to 10% of adults at some point in their lives. Like achilles tendinopathy, the name is somewhat misleading — chronic plantar fasciitis is more accurately a degenerative process (fasciosis) than a purely inflammatory one. The fasciosis root cause is primarily due to muscle dysfunction.
Plantar Fasciitis Symptoms
- Sharp, stabbing pain on the bottom of the heel — especially with first steps in the morning
- Pain that improves with movement but returns after prolonged standing or walking
- Tenderness when pressing directly under the heel bone
- Pain that may radiate into the arch
- Worsening pain after (not usually during) periods of activity
Risk Factors
- Prolonged standing, especially on hard surfaces (teachers, nurses, factory workers, retail professionals)
- Obesity or being overweight — one of the strongest risk factors
- High arches or flat feet — both alter how load is distributed across the fascia
- Tight calves and Achilles tendon — yes, they are connected (more on this below)
- Improper footwear — wearing shoes with arch support, wearing orthotics, not wearing zero drop shoes
- Age 40–60 — the peak incidence range, though much more common in a younger population recently
What About Heel Spurs? |
Side-by-Side Comparison — Achilles Tendonitis vs. Plantar Fasciitis
This table breaks down the key differences to help you determine whether you’re dealing with Achilles tendonitis or plantar fasciitis. Use it as a reference, but remember — a proper clinical evaluation is essential for an accurate heel pain diagnosis.
Feature | Achilles Tendonitis | Plantar Fasciitis |
|---|---|---|
Pain location | Back of heel / lower calf (along the tendon) | Bottom of heel / arch |
Structure affected | Achilles tendon (connects calf muscles to heel bone) | Plantar fascia (supports the arch, runs heel to toes) |
Morning pain pattern | Stiffness and aching that “warms up” with movement | Sharp, stabbing pain with first steps; eases then returns |
Pain after rest | Stiffness when getting up after prolonged sitting | Sharp pain with first steps after sitting |
Pain with activity | Increases during/after running, jumping, pushing off | Increases with prolonged standing and walking |
Swelling | Often visible along the tendon or at the heel | Rarely visible |
Tenderness location | Squeeze the tendon at the back of the ankle/heel | Press the bottom of the heel (medial calcaneal tubercle) |
Common in | Runners, athletes, active adults | Standing professionals, overweight individuals, age 40–60, runners |
Footwear effect | Rigid heel counters aggravate it (especially insertional) | Flat shoes and barefoot walking feel worse |
Stretch test | Pain with dorsiflexion (pulling toes up stretches the tendon) | Windlass test — pain when big toe is pulled back, stretching the fascia |
Bone involvement | Insertional type may have Haglund’s deformity or calcifications | Heel spur may be present (usually not the pain source) |
Best initial treatment | Eccentric loading (Alfredson protocol for mid-portion) | Stretching, arch support, plantar fascia-specific loading |
The Tricky Part — Why These Get Confused
If you’re wondering “do I have achilles tendonitis or plantar fasciitis?”, you’re asking a question that even some healthcare providers get wrong. Here is why these two conditions create so much diagnostic confusion:
- Both cause heel pain. The word “heel” is doing a lot of heavy lifting — it can mean the back, bottom, or sides of the calcaneus.
- Both cause morning stiffness. That question — “heel pain in the morning: Achilles or plantar fasciitis?” — is one of the most common we field. Both conditions present with morning symptoms, but the quality of that pain differs (stiff and achy vs. sharp and stabbing).
- Both are worse after rest and with increased acutely increased activity levels.
- Both are overuse/degenerative conditions — not truly inflammatory despite the “-itis” suffix. Chronic cases involve collagen disorganization, not active inflammation.
But here is the most important reason these conditions get confused: the achilles tendon and plantar fascia are anatomically connected. The achilles tendon fibers wrap around the calcaneus and blend directly into the plantar fascia. They function as a continuous chain. Tightness or dysfunction in one structure directly increases stress on the other. This anatomical reality explains why a tight achilles/calf complex is a risk factor for both conditions — and why insertional Achilles tendonitis and plantar fasciitis can co-exist, sharing the calcaneus as their common attachment point.
Can You Have Both at the Same Time?
Yes — and it is more common than most people realize.
The anatomical connection between the Achilles tendon and plantar fascia through the calcaneus means dysfunction in one structure can directly stress the other. A chronically tight Achilles tendon increases load on the plantar fascia with every step. Conversely, chronic plantar fascia stiffness can alter gait mechanics and overload the Achilles.
If you have pain on the bottom AND back of your heel, you may have both conditions simultaneously — and both need to be addressed. This is exactly why a comprehensive biomechanical evaluation matters. Looking only at the painful spot and ignoring the rest of the kinetic chain is a recipe for incomplete treatment and persistent symptoms.
Clinical Insight |
Simple At-Home Tests (Before You See a Specialist)
These practical self-assessment tests can help you start narrowing down whether your heel pain is coming from the Achilles tendon, the plantar fascia, or both. Use them as screening tools before scheduling a professional evaluation.
1. The Squeeze Test (Achilles Tendonitis)
- Sit on a chair and extend your affected leg in front of you.
- Squeeze the Achilles tendon between your thumb and forefinger, starting about 2 inches above the heel bone and moving upward along the tendon.
- Pain with squeezing = likely Achilles tendonitis.
- Check for thickening, a nodule, or a “bump” in the tendon — a sign of chronic tendinopathy.
2. The Press Test (Plantar Fasciitis)
- Cross your affected foot over your opposite knee.
- Press firmly on the bottom of your heel, specifically the inner (medial) side where the plantar fascia attaches.
- Sharp pain at the heel’s bottom = likely plantar fasciitis.
3. The First-Step Test
- Pay attention to how your heel feels with the very first steps in the morning.
- Sharp, stabbing pain on the bottom of the heel = classic plantar fasciitis presentation.
- Stiff, achy pain at the back of the heel/ankle = classic Achilles tendonitis presentation.
- Both? You may have both conditions.
4. The Windlass Test (Plantar Fasciitis–Specific)
- While seated, pull your big toe back toward your shin, stretching the plantar fascia.
- If this reproduces your pain on the bottom of the foot, plantar fasciitis is very likely.
Important Disclaimer |
How Treatment Differs — And Why the Right Diagnosis Matters
This is the section that matters most. The difference between Achilles tendonitis and plantar fasciitis is not academic — it directly determines which treatment protocol will help you and which will waste your time or make things worse.
Treatment for Achilles Tendonitis
- Eccentric loading – The Alfredson protocol is the gold standard for mid-portion Achilles tendinopathy — progressive heel-drop exercises that stimulate tendon remodeling by loading the tendon in a lengthened position. Our secret is that we can get you doing them pain free usually within the first 7 days while other methods take months and months.
- Modified loading for insertional cases: Aggressive heel drops can actually worsen insertional Achilles tendonitis by compressing the tendon against the bone. The protocol must be adapted, which is why we get the pain gone fast!
- ARPwave therapy — a neurological muscle re-education system that identifies and corrects the compensation patterns in the brain that are driving tendon overload. Rather than just treating the painful tendon, ARPwave locates the nerves that have shut off the muscles. This repairs the muscles failing to absorb force properly and retrains them. This is a key differentiator in our clinic. (only in our Mesa clinic, not Scottsdale)
- Biomechanical correction of the entire kinetic chain — addressing calf tightness, ankle mobility deficits, hip and glute weakness, and running/jumping mechanics.
Treatment for Plantar Fasciitis
- Plantar fascia–specific strengthening and loading protocols — including the high-load strength training protocol that has shown superior outcomes to traditional stretching alone.
- Appropriate footwear guidance — crucial for reducing fascial strain during daily activities. Converting to zero-drop shoes as fast as possible will keep the plantar fasciitis from returning later.
- Soft tissue mobilization of the plantar fascia and the calf complex when needed.
- Addressing calf and achilles tightness — the upstream driver. If the calf is tight, this means it can no longer absorb force and the fascia takes excessive load with every step.
Why Getting This Right Matters
Wrong Diagnosis = Wrong Treatment = Worse Outcomes Consider these common mismatches: • The Alfredson eccentric heel-drop protocol — the gold standard for mid-portion Achilles tendonitis — can worsen insertional Achilles tendonitis AND does nothing meaningful for plantar fasciitis. • Aggressive arch support helps plantar fasciitis but does not address Achilles tendon pathology. • Stretching the plantar fascia feels good, but stretching the Achilles in certain ways can aggravate insertional tendonitis. • Generic “rest and ice” advice helps neither condition long-term — both require progressive loading to stimulate tissue remodeling. |
Bottom line: Wrong diagnosis = wrong treatment = wasted time, wasted money, and potentially making your condition worse. This is why a provider who understands the biomechanical relationship between these structures — and who can differentiate between them on exam — is critical.
When to See a Specialist for Your Heel Pain
Self-care has its limits. Schedule a professional heel pain diagnosis in Mesa, AZ (or wherever you are) if any of the following apply:
- Pain that has persisted more than 2–4 weeks despite rest and basic home care
- Morning pain that is getting worse, not better, over time
- Pain that limits your ability to be a freaking champion
- Swelling, visible changes to the tendon, or a bump on the back of your heel
- Previous treatment that isn’t working — heel pain is highly treatable by experienced clinicians
- A sudden “pop” or acute sharp pain in the back of the heel or calf — this could indicate an achilles rupture and requires immediate evaluation
Don’t Ignore a Possible Rupture If you experienced a sudden, sharp pain in the back of your heel or calf — especially during explosive activity — accompanied by difficulty walking or pushing off, seek evaluation immediately. Achilles tendon ruptures require urgent care and have significantly better outcomes with early intervention. |
Get the Right Diagnosis — Stop Guessing, Start Healing
The difference between Achilles tendonitis and plantar fasciitis is not subtle — but it requires a provider who actually examines the right structures and understands the biomechanical connection between them. A quick glance at your heel and a generic prescription for “rest and stretching” is not a diagnosis. It is a guess.
Dr. Houston Anderson is a functional medicine doctor, chiropractor, and sports rehab specialist who differentiates conditions through comprehensive biomechanical evaluation, assesses the full kinetic chain from your feet through your hips, and creates condition-specific treatment plans — not one-size-fits-all protocols.
We treat both conditions daily in our Mesa, AZ clinic using ARPwave therapy, PEMF therapy,laser therapy and advanced evidence-based rehabilitation protocols designed to get you back to the activities you love — running, training, pickleballing and winning championships!
Ready to Get Answers? Call 480) 331-9554 to schedule a free phone consultation. Proudly serving Mesa, Gilbert, Chandler, Tempe, Scottsdale, and the greater East Valley. |
Leave a Reply